Lung Adenocarcinoma Symptoms Often Spotted at Late Stage, Treatment Options Available
Lung cancer is the leading cause of cancer deaths, with the highest mortality worldwide. Specifically, adenocarcinoma is the most common, which shows no obvious symptoms and may have reached an advanced stage when detected. However, updated treatments may help improve a patient’s condition or even cure it.
Symptoms of Advanced Lung Adenocarcinoma Are Not Obvious
With the highest incidence rate globally among cancers, lung cancer falls into small cell lung cancer and non-small cell lung cancer, which includes squamous cell carcinoma and adenocarcinoma.
While small cell lung cancer and squamous cell carcinoma are closely associated with smoking, more than half of the world’s lung cancer patients are victims of adenocarcinoma, which is not necessarily related to smoking.
In its early stage, adenocarcinoma does not cause feeling for patients because the condition tends to occur in the periphery of the lung, surrounded by lung tissues where there is no pain nerve, rather than close to the edge of the lung (or near the pleural area), or in the mid-thorax.
No symptom will appear until a cancer mass grows large enough to pose pressure on other tissues such as bigger tracheae and lung walls, by this time the condition is usually found to be already in an advanced stage.
Therefore, the only way to detect early-stage lung adenocarcinoma is to use CT tomography for screening rather than diagnosing based on symptoms.
Small cell lung cancer, mostly located near the mid-thorax, grows rapidly and metastasizes easily. Patients may respond well to initial treatment but will soon become resistant to drugs and can no longer find other effective treatments easily.
Lung adenocarcinoma tends to grow in the peripheral lung while squamous cell carcinoma grows in the mid-thorax. In recent years, most of the latest treatment advances in lung cancer focus on non-small cell lung cancer, with many successful cases surviving more than five years.
Adenocarcinoma Often Found Late, Higher Cases Among Female Non-Smokers
The past few years have seen significant changes in the incidence rate of lung cancer by gender. Previously, male patients outnumbered female ones due to a higher tobacco smoking rate.
However, the rates of lung cancer in men and women are getting closer in countries with small proportions of smokers.
Non-smokers account for more than half of the women with lung cancer.
Why is adenocarcinoma often found late and seen more among female non-smokers? The causes remain unidentified. Common contributing factors include secondhand smoke, polluted air (e.g., PM2.5), and cooking fumes.
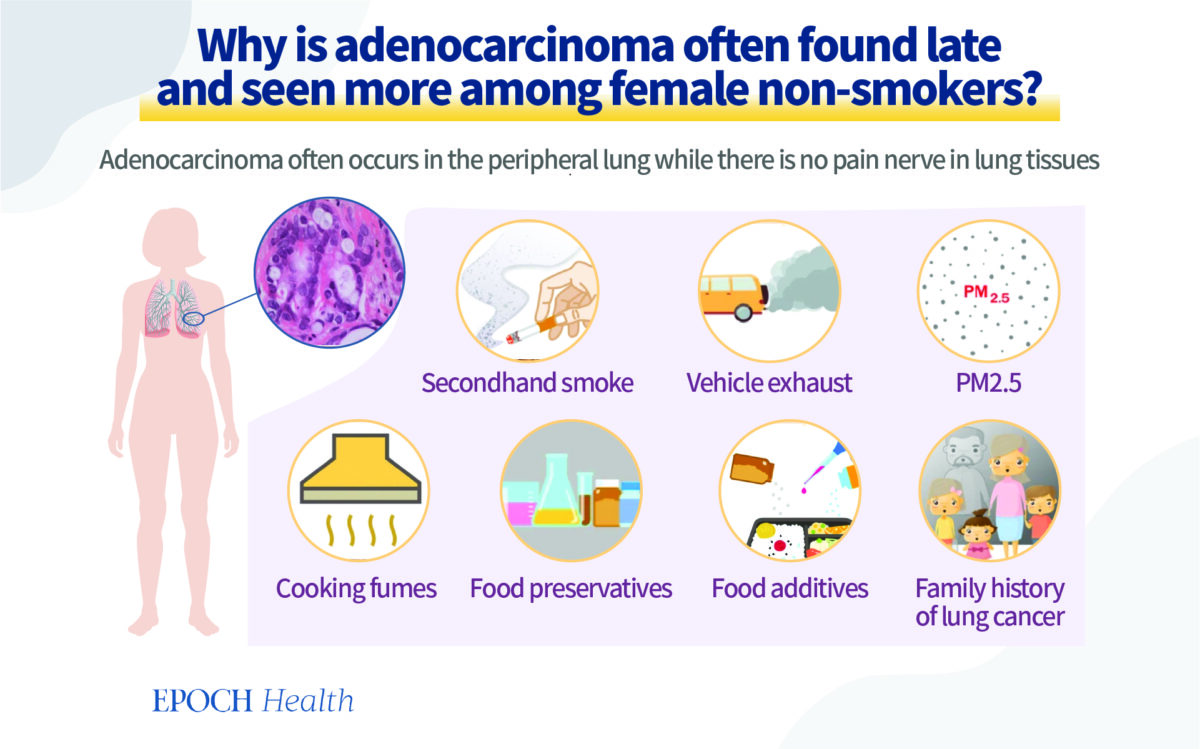

Recent studies also suggest those with a family history of lung cancer found among three-generation relatives have a higher chance of developing it, especially in women, which may be related to genetics.
An environmental cause is the use of preservatives and additives. New studies in Taiwan showed that such substances led to genetic mutation; and that the more people were exposed to them, the more they were likely to suffer from cancer.
The above factors may explain why non-smokers also develop lung cancer. Women may have greater chances of being exposed to those risk factors. Some assume lung cancer is associated with female hormones, which lacks exact supporting evidence so far. However, those risk factors should be avoided or heeded as much as possible.
Targeted Therapy and Immunotherapy Thriving in Lung Cancer Care
If lung cancer is detected early, surgery is the best solution. If a tumor mass is large or has spread to lymph nodes, chemotherapy or radiotherapy will be needed as an auxiliary means. In the case of cancer metastasis making surgery impossible, systemic treatment will be the main choice left, such as chemotherapy, targeted therapy, and immunotherapy.
There have been many advances in the treatment of non-small cell lung cancer over the years, featuring targeted therapy and immunotherapy.
However, the strategy for the treatment of small cell lung cancer is different because patients have little chance of surgical removal due to possible metastasis, even if the tumor is small in size.
The primary cure for small cell lung cancer is chemotherapy, together with radiotherapy when necessary. Latest studies show that the combination of immunotherapy and standard chemotherapy is effective in extending the lives of patients.
Historically, lung cancers, regardless of their types, were treated the same way in the early stages because the treatments available were quite limited.
Findings show that even for the same type of lung cancer, the condition varies from patient to patient, especially in the event of gene mutation. So, corresponding targeted therapy can be created based on individual mutations. In other words, a patient with mutation A is a candidate for type A targeted therapy while another patient with mutation B is a candidate for type B targeted therapy.
Mutated genes vary from patient to patient, requiring different drugs. This is where precision medicine comes in.
With precision medicine, cancer patients have a high chance of effective treatment. For example, under a non-personalized treatment, two to three out of every 10 patients may receive effective treatment. However, under precision therapy, seven to eight of them may be well treated and avoid side effects that are caused by unnecessary drugs.
More Than Half of Lung Cancer Patients Candidates for Targeted Gene Therapy
Whenever there is cancer, there must be gene mutation and, likely more than one gene involved.
In one well-known, influential study, researchers divided lung adenocarcinoma patients into two groups, EGFR (epidermal growth factor receptor) mutation-positive and negative, and provided patients with targeted drugs that inhibited EGFR gene mutation.
If a corresponding mutation occurs, it shows that patients are more responsive to targeted drugs and will survive longer. Conversely, if no corresponding mutation occurs, it means they respond better to conventional chemotherapy and will survive longer, too.
In today’s era of precision treatment for lung cancer, doctors often ask patients to first take a test. Only when patients have a specific genetic mutation will doctors use gene-targeted drugs to treat them.
Clinical trials have proven that roughly 60 percent of all lung cancer patients are candidates for gene-targeted therapy.
The success or failure of gene-targeted therapy relies on different gene mutations and drugs corresponding to them, as well as the timing of drug administration. Broadly speaking, if applied early enough, the treatment efficiency rate can reach 70 to 80 percent.
For example, a 41-year-old woman with stage IV lung adenocarcinoma had metastases to bone and brain. She was EGFR mutation-positive. Her symptoms improved significantly on the third day since the start of targeted therapy.
An X-ray image showed her tumor was no longer visible on the seventh day.
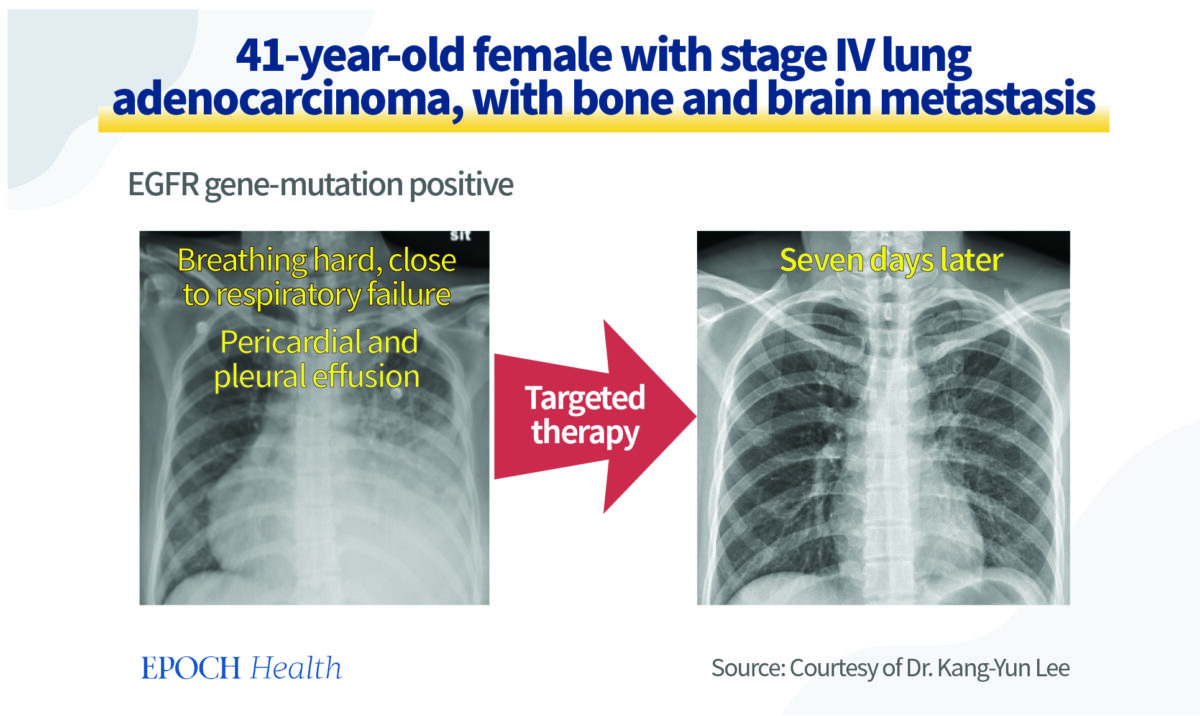

In fact, some symptomatic targeted drugs work within days. Most patients will have minimal tumors after taking them for one to three months. Gene-targeted therapy is a quick and effective treatment, which also makes patients comfortable.
Although targeted therapy can reduce the size of tumors, it cannot eradicate all cancer cells. Except for a small number of lucky patients whose cancer cells can be removed, the vast majority of patients have to take medication for a long time, like those with high blood pressure.
Immunotherapy Carries Minimal Side-Effects
Immune checkpoint inhibitor therapy is the best immunotherapy method available.
The human body’s immune cells—T cells—can distinguish between pathogens or cancer cells and remove them.
In this process, immune screening allows T cells to distinguish between the “good guys” (normal cells) and “bad guys” (pathogens, cancer cells, etc.) in the body. If immune cells attack all cells indiscriminately, people will fall sick.
Cancer cells can trick T cells into thinking that they are normal cells and thus avoid being attacked.
Immunotherapy is moving toward precision treatment: scientists have designed a drug that allows T cells to re-identify and remove cancer cells.
Immunotherapy is appropriate if a lung cancer patient’s cancer cells contain a high percentage of PD-L1 molecular expression.
For example, a 72-year-old male with stage IV lung adenocarcinoma found no gene-targeted therapy suitable for him after genetic tests. However, a PD-L1 test revealed that his cancer cells had up to 85 percent of PD-L1 expression, making him a good candidate for immunotherapy.
After long-term treatment, his lung cancer was effectively brought under control and has not recurred.
Currently, all lung cancer patients can find suitable immunotherapy treatments with different combinations of drugs.
People associate conventional chemotherapy with side effects like nausea, vomiting, hair loss, and lower white blood cell count. But immunotherapy is not the case.
Firstly, only 30 percent of immunotherapy patients experience side effects while most show no side effects at all.
Secondly, only about 10 percent of patients have serious side effects in the case of immunotherapy, though side effects may occur in any bodily organ, causing hepatitis, thyroid or neurological inflammation, or interstitial pneumonia. Furthermore, these side effects are likely to be avoided with close monitoring and early preventive steps.
What Is Dual Immunotherapy?
Immune checkpoint inhibitors are effective immunotherapeutic drugs available, mainly consisting of two types of inhibitors.
Most lung cancer patients need only one type of inhibitor while a limited number of patients need both, i.e., dual immunotherapy, to achieve beneficial outcomes.
That is because, if we compare T cells that remove cancer cells in the body to a car charging forward, the situation of some patients is the same as using both the foot and hand brakes, thus making the vehicle unable to run forward with full power. However, dual immunotherapy is meant to release the two brakes as in the T cells at the same time, allowing them to attack and eliminate cancer cells in full play.
There are also some patients who have to use both immune checkpoint inhibitors and chemotherapeutic drugs to achieve desirable results.
Clinical Trials Are Optional When Existing Therapies Fail
All drugs that are approved for lung cancer treatment have gone through clinical trials. Countless clinical trials are underway around the world.
Many physicians actively seek suitable clinical trials while cancer patients receive standard treatment.
Let’s take a 69-year-old female with adenocarcinoma as an example. Genetic testing found her not a candidate for gene-targeted therapy. Her tumor recurred and escalated so much that there was no longer standard treatment for her due to her previous chemotherapy and immunotherapy. Later, the patient joined a clinical trial program concerning an antibody-drug conjugate and succeeded. She eventually recovered and returned to her favorite job.
Antibody-drug conjugate is an important trend in current anti-cancer drug research. It allows drugs to concentrate at the tumor site and to kill cancer cells without harming normal cells.
How to Prevent Lung Cancer Recurrence
Lung cancer patients’ five-year survival rate and postoperative recurrence rate vary with the stages they are in. Overall, early-stage patients have a higher survival rate and a lower recurrence rate while advanced-stage patients are in the opposite situation.
Post-surgery adjuvant therapy treatment with gene-targeted drugs can reduce cancer recurrence.
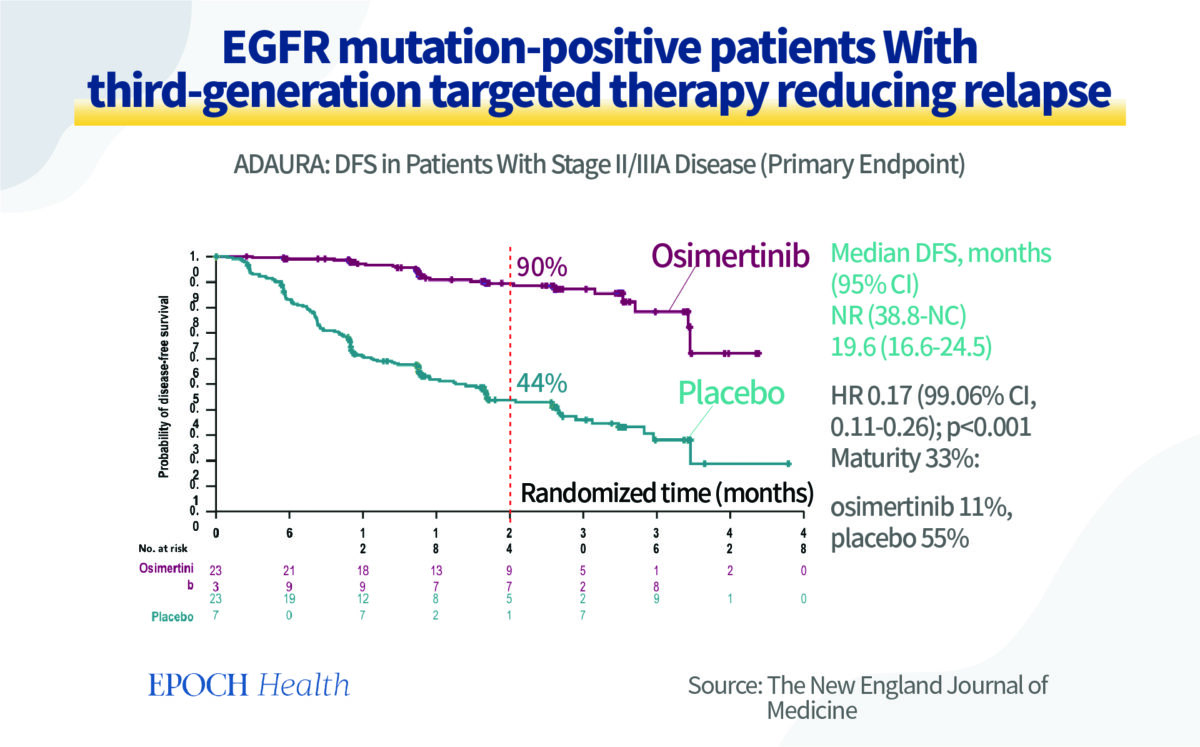
A 2020 study in the New England Journal of Medicine shows that patients with EGFR mutation-positive cancer could effectively reduce recurrence after receiving surgery, chemotherapy, and three consecutive years of gene-targeted drugs.
At two years, the relapse-free survival rate was 90 percent for the drug-treated group but 44 percent for the control group. At three years, the relapse-free rate still stayed close to 80 percent for the drug-treated group but about one-third for the control group.

If no EGFR gene mutation is seen in cancer patients, doctors can also use immunotherapy to reduce recurrence, which large-scale clinical studies have corroborated.
Chemotherapy and immunotherapy, either preoperative or postoperative, can be effective in preventing lung cancer from returning.
Another success story is a 60-year-old male with stage II lung adenocarcinoma. He received chemotherapy and immunotherapy prior to surgery. Following his tumor removal, a test showed all his cancer cells had been destroyed. Now, more than two years after his surgery, his cancer has not returned.
Such cases are many. To date, immunotherapy before or after surgery has become standard care for lung cancer, playing a major role in preventing recurrence.
Epoch Health articles are for informational purposes and are not a substitute for individualized medical advice. Please consult a trusted professional for personal medical advice, diagnoses, and treatment. Have a question? Email us at [email protected]

Follow
Kang-Yun Lee is a doctor at Shuang Ho Hospital in Taiwan.
Follow
" Conservative News Daily does not always share or support the views and opinions expressed here; they are just those of the writer."